When a doctor prescribes a medication like warfarin, digoxin, or phenytoin, the difference between a safe dose and a dangerous one can be razor-thin. These are NTI drugs - Narrow Therapeutic Index drugs - and they demand far more precision than most generics can deliver. The FDA doesn’t treat them like ordinary medications. If a generic version of an NTI drug doesn’t meet exacting standards, it won’t get approved. And for patients, that means more than just a cheaper pill - it means avoiding life-threatening mistakes.
What Makes a Drug an NTI Drug?
Not all drugs are created equal when it comes to safety margins. The FDA defines an NTI drug using a clear, data-driven cutoff: a therapeutic index of 3 or less. That means the dose that causes toxicity is no more than three times the dose that works. For context, most drugs have a therapeutic index of 10, 20, or even higher. With NTI drugs, a 10% variation in blood concentration can mean the difference between effective treatment and toxic overdose.The FDA identified this threshold through pharmacometric analysis of 13 key drugs in 2022. Ten of them had a therapeutic index of 3 or lower. Three others hovered just above it - but still required stricter controls due to other risk factors like narrow dosing increments or the need for frequent blood monitoring.
Common NTI drugs include:
- Carbamazepine (for epilepsy)
- Phenytoin (another antiseizure drug)
- Warfarin (blood thinner)
- Digoxin (heart medication)
- Valproic acid (mood stabilizer)
- Tacrolimus and cyclosporine (immunosuppressants)
- Lithium carbonate (for bipolar disorder)
These aren’t rare or obscure drugs. They’re used daily by hundreds of thousands of patients. And because they’re so sensitive, even small differences between brand and generic versions can trigger serious side effects - seizures, bleeding, organ rejection, or cardiac arrhythmias.
How the FDA Tests Bioequivalence for NTI Drugs
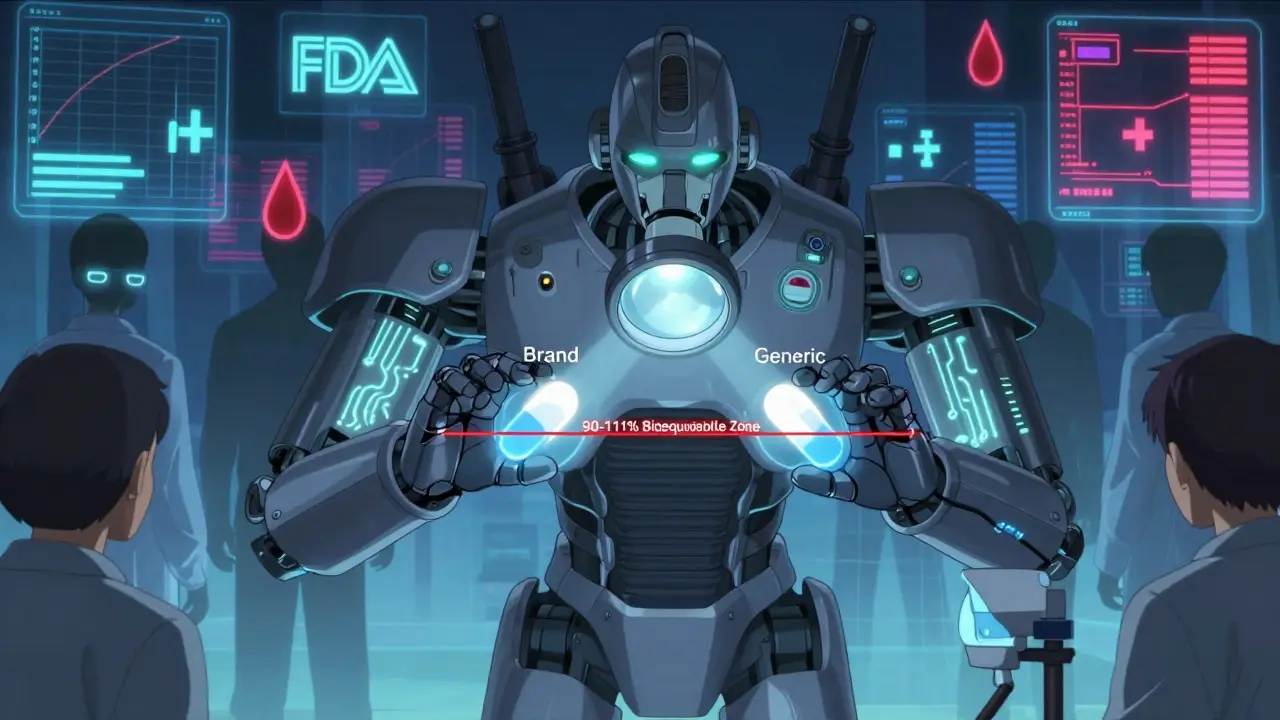
For regular generic drugs, the standard bioequivalence test requires the generic to deliver 80% to 125% of the brand’s drug exposure in the bloodstream. That’s a 45% window. For NTI drugs? That window shrinks to 90% to 111%. That’s less than half the range.This isn’t just a suggestion. It’s a hard requirement. To get approved, a generic NTI drug must pass two tests:
- Average Bioequivalence (ABE): The average drug levels must fall between 90% and 111% of the brand.
- Reference-Scaled Average Bioequivalence (RSABE): The variability between doses must be tightly controlled. The upper limit of the 90% confidence interval for the ratio of within-subject variability (test vs. reference) must be ≤ 2.5.
Why two tests? Because some NTI drugs have high variability in how people absorb them. If you only used the 90-111% rule, a drug with high variability might slip through. The RSABE rule forces manufacturers to prove their product doesn’t swing too wildly from dose to dose - even if the average looks fine.
Studies must also be replicate designs. That means each patient takes both the brand and generic versions multiple times - often in a crossover pattern like ABBA or BABA. This gives regulators enough data to measure within-person variability accurately. Standard two-period studies (one dose of brand, one of generic) aren’t enough.
Quality Control Is Tighter Too
Bioequivalence isn’t just about what’s in the bloodstream. The FDA also tightens quality control for NTI drugs.For regular generics, the active ingredient must be 90% to 110% of the brand’s amount. For NTI drugs? That range is cut in half: 95% to 105%. That’s a 10% tolerance - not 20%. It means the manufacturing process must be incredibly consistent. A single batch can’t vary more than 5% above or below the target.
This level of precision demands advanced manufacturing, real-time monitoring, and rigorous quality assurance. It’s one reason why so few generic manufacturers bother with NTI drugs. The cost and complexity are high. But for patients, it’s worth it.
Why This Matters in Real Life
Imagine a transplant patient on tacrolimus. Their body rejects the new organ if the drug level drops too low. It causes kidney damage or seizures if it rises too high. Their doctor carefully adjusts the dose based on weekly blood tests. Now, switch to a generic version that’s technically “bioequivalent” under old standards - but doesn’t meet the 90-111% rule.Even if the average concentration looks fine, the variability might be higher. One day, the patient gets 115% of the expected dose. The next day, 85%. That rollercoaster could mean hospitalization. The FDA’s stricter standards prevent that.
Real-world data supports this. Studies of generic tacrolimus in transplant patients show that when the 90-111% rule is applied, patients maintain stable drug levels. The same can’t be said for generics that only meet the 80-125% standard. In fact, some generic versions of NTI drugs that passed the old test were later found to be non-equivalent to each other - even though each met FDA requirements at the time.
Why the FDA Doesn’t Publish a Public List
You won’t find a single, official list of all NTI drugs on the FDA website. Instead, the agency assigns NTI status case-by-case through product-specific guidance documents. Why? Because the therapeutic index isn’t the only factor. A drug’s dosing pattern, monitoring needs, and clinical history matter too.For example, lithium has a therapeutic index of about 2.5 - clearly an NTI drug. But phenytoin’s index is closer to 3.2. Still, because it requires frequent blood tests and has a history of substitution-related seizures, it’s treated as an NTI drug. The FDA looks at the whole picture, not just a number.
This approach gives regulators flexibility. But it also creates confusion. Pharmacists, especially outside major hospitals, often don’t know which drugs are NTI. Some states still require patient consent before substituting a generic for an NTI drug - even if the FDA says it’s safe. Education is lagging behind science.
Global Differences and Ongoing Challenges
The FDA’s scaled approach - using both ABE and RSABE - is more sophisticated than what other agencies use. Health Canada and the EMA typically just tighten the bioequivalence range to 90-111% without scaling for variability. That’s simpler, but less precise. It might allow some variable products to pass, or block some truly equivalent ones.The FDA acknowledges this gap. It’s pushing for global harmonization. But until that happens, manufacturers must tailor their submissions to each region. A generic approved in the U.S. might not get approved in Europe - and vice versa.
Another challenge? Antiepileptic drugs. Despite FDA approval, many neurologists remain cautious. Some studies show no difference between brand and generic carbamazepine. Others show increased seizure frequency after switching. The science isn’t perfect. But the FDA’s position is clear: if a generic meets the 90-111% rule and passes RSABE, it’s therapeutically equivalent. Real-world evidence from millions of prescriptions supports that.
What Patients Should Know
If you take an NTI drug - whether brand or generic - keep these points in mind:- Don’t switch between generic brands without consulting your doctor. Even if both are FDA-approved, small differences in formulation can affect you.
- Stick to the same pharmacy. Different manufacturers use different fillers and coatings. Consistency matters.
- Monitor symptoms. If you feel different after a refill, tell your doctor. Blood tests may be needed.
- Ask if your generic meets NTI standards. Most do - but not all.
The FDA’s standards for NTI drugs aren’t about blocking generics. They’re about making sure generics are safe. And they work. Since the stricter rules took effect, adverse events linked to NTI drug substitutions have dropped. The system isn’t perfect - but it’s the best we have.
What drugs are considered NTI drugs by the FDA?
The FDA doesn’t publish a public list, but common NTI drugs include carbamazepine, phenytoin, warfarin, digoxin, valproic acid, tacrolimus, cyclosporine, sirolimus, and lithium carbonate. These are identified through product-specific guidance documents based on therapeutic index, dosing precision, and clinical history.
Why are the bioequivalence limits for NTI drugs tighter than for other drugs?
Small changes in blood concentration of NTI drugs can lead to serious side effects or treatment failure. A 20% difference in exposure that’s acceptable for most medications could be dangerous for drugs like warfarin or digoxin. The FDA’s 90-111% range reduces this risk by limiting variability and ensuring consistent performance.
Do generic NTI drugs work as well as brand-name versions?
Yes - if they meet the FDA’s stricter NTI standards. Generic NTI drugs approved under the 90-111% bioequivalence range and RSABE criteria are considered therapeutically equivalent to their brand-name counterparts. Real-world data from transplant and epilepsy patients supports this. However, switching between different generic brands without medical supervision is not recommended.
What is RSABE and why is it used for NTI drugs?
RSABE stands for Reference-Scaled Average Bioequivalence. It’s a statistical method that adjusts bioequivalence limits based on how variable the brand-name drug is in the body. For NTI drugs, this prevents products with high variability from being approved, even if their average concentration looks good. It ensures both consistency and safety.
Can I safely switch between generic versions of an NTI drug?
It’s not recommended without medical oversight. Even though each generic meets FDA standards, differences in excipients, manufacturing processes, or dissolution profiles can affect absorption. Patients on drugs like tacrolimus or phenytoin should stick to the same manufacturer unless their doctor approves a switch - and even then, blood levels should be monitored.


Denise Jordan
March 9, 2026 AT 18:05I don't get why we need all this fancy math just to approve generics. My pharmacist swaps my warfarin brand every other refill and I'm fine. If it's the same pill, why does it matter who made it?
Also, I swear the last batch made my legs feel like lead. Probably just stress.
Gene Forte
March 10, 2026 AT 18:34This is exactly the kind of thoughtful, science-driven policy that makes the FDA worth trusting. We don't need to cut corners on drugs that can kill you with a single wrong dose. The 90-111% standard isn't bureaucracy-it's basic human responsibility.
Every patient deserves consistency. Not just cheaper pills. Real safety. And that's what this system delivers.
Kenneth Zieden-Weber
March 12, 2026 AT 12:45So let me get this straight-we're saying a drug that kills you if it's 10% off needs a 2% tighter window than your average ibuprofen?
That's not overkill. That's math. And honestly? I'm impressed. Most people think 'generic = same' but they don't realize the difference between 85% and 115% in your bloodstream is the difference between breathing and being intubated.
Good job, FDA. Now if only pharmacies would stop auto-substituting without telling patients...
Chris Bird
March 14, 2026 AT 07:08This is just corporate control. Big Pharma doesn't want generics to compete. So they made up fake science to scare people. The '90-111%' rule? Total nonsense. I've seen people switch and do fine. They're just milking the system.
David L. Thomas
March 16, 2026 AT 03:09The RSABE framework is a game-changer. Traditional ABE fails spectacularly for high-variability NTI drugs-especially tacrolimus and cyclosporine. The scaled approach accounts for intrinsic PK variability, which is critical when you're dealing with drugs that have nonlinear absorption and narrow margins.
And yes, replicate designs aren't optional. You need within-subject variance data to properly estimate the upper confidence bound. Otherwise you're flying blind.
LiV Beau
March 17, 2026 AT 13:17I'm so glad someone finally explained this clearly 😊
My mom's on lithium and we switched generics once and she got really shaky for a week. We went back to the original and boom-stable again. No one told us about the differences between manufacturers. This is life-or-death stuff. Thank you for the breakdown!
Adam Kleinberg
March 19, 2026 AT 00:59They say they're protecting us but really they're protecting Big Pharma's profits
Who even decided on 90-111 why not 88-113 why not 95-105
It's all arbitrary
And don't get me started on replicate designs they're just making it harder for generics to enter the market
They want you to pay $500 a month for a pill that costs 2 cents to make
Bridgette Pulliam
March 21, 2026 AT 00:22The fact that pharmacists aren't consistently trained on NTI drug substitution is alarming. I work in a hospital pharmacy and even we have to cross-check product-specific guidance documents for each drug. Many community pharmacies don't have access to those.
There needs to be a centralized, updated, publicly accessible database-not just scattered FDA guidances. Patients shouldn't have to become pharmacologists to stay safe.
Mike Winter
March 22, 2026 AT 21:13I appreciate the nuance here. The FDA's case-by-case approach acknowledges that biology doesn't fit neatly into boxes. A therapeutic index of 3.2 doesn't automatically disqualify phenytoin from NTI status-because clinical outcomes matter more than numbers on a spreadsheet.
Still, I wonder if global harmonization might be better served by adopting a tiered system: basic bioequivalence for low-risk drugs, and RSABE+ for high-risk. That way we don't over-regulate everything.